

DR DOUG QUARRY and PROFESSOR JOHN OXFORD
EXECUTIVE SUMMARY
- Coronavirus does not have a brain
- When it comes to COVID-19 vaccines, rich nations are first in line
- Another dose of vaccines
- A Tweetorial on pre-existing immunity from @AdamKucharski
- Pre-existing immunity
- Mis / Dis-information / Fake news
- Journal / Article / Twitter roundup
- Air in the hospital room of COVID-19 patients is infectious
- A View from the Lab: Professor John Oxford
CORONAVIRUS DOES NOT HAVE A BRAIN
“It’s brutal in its simplicity. It’s brutal in its cruelty. But it doesn’t have a brain. We have the brains. We can outsmart something that doesn’t have a brain, but we’re not doing such a great job right now,”
Mike Ryan, Director of WHO’s Health Emergencies Programme
“There are many, many things that we can do right now to outsmart this virus. While work on therapeutics and vaccines will continue, at this point chains of transmission can be broken. These include social distancing, contact tracing, quarantining infected individuals, the use of masks when physical distancing isn’t possible, and hand washing. “If we do all of these things, we can outsmart the virus, and we can prevent this virus from passing from one individual to another. Everyone on the planet needs to understand that they have a role to play in breaking the chain of transmission.”
Maria Van Kerkhove, WHO’s Technical Lead for Coronavirus
WHEN IT COMES TO COVID-19 VACCINES, RICH NATIONS ARE FIRST IN LINE
Wealthy countries have already locked up more than a billion doses of coronavirus vaccines, raising worries that the rest of the world will be at the back of the queue in the global effort to defeat the pathogen.
- Although international groups and a number of nations are promising to make vaccines affordable and accessible to all, doses will likely struggle to keep up with demand in a world of roughly 7.8 billion people
- The possibility wealthier countries will monopolize supply – a scenario that played out in the 2009 swine flu pandemic – has fueled concerns among poor nations and health advocates
SUMMARY OF COVID-19 VACCINE PRE-PURCHASES
| OXFORD / ASTRA ZENECA(UK) | MODERNA / NIAID(USA) | PFIZER & BioNTECH(Germany) | SANOFI GLAXO(UK) | NOVAVAX(USA) | VALVNA(France) | JANNSEN / JOHNSON & JOHNSON(BELGIUM / USA) | SERUM INSTITUTE OF INDIA | |
| GAVI / COVAX * | 300 million doses | INTEREST | Sub-license to produce 400 million doses of Oxford / AstraZeneca ** | |||||
| USA | $1.2 billion300 million doses? available Oct 2020 | $1.53 billion100 million dosesOption of 400 million more doses | $1.95 billion100 million dosesOption of 500 million more doses | $1.95 billion | $1.6 billion | $1 billion100 million dosesOption for 200 million more doses | ||
| EU*** | 400 million doses | 300 million doses | ||||||
| UK | 30 million doses? available Sept 2020 | 30 million doses | 60 million doses |
* The World Health Organization, the Coalition for Epidemic Preparedness Innovations (CEPI), and GAVI, the Vaccine Alliance, are working together to bring about equitable and broad access. They outlined an $18 billion plan in June to roll out shots and secure two billion doses by the end of 2021. The initiative, known as Covax, aims to give governments an opportunity to hedge the risk of backing unsuccessful candidates and give other nations with limited finances access to shots that would be otherwise unaffordable. IVA and CEPI/GAVI say AstraZeneca will supply the vaccine at no profit during the pandemic
**AstraZeneca has signed an agreement with the Serum Institute of India to sub-license the Oxford vaccine to supply one billion doses to low- and middle-income countries, with a commitment to provide 400 million by year end
*** The EU purchases via the Inclusive Vaccines Alliance (IVA), set up by Germany, France, Italy, and the Netherlands
THE IMPERIAL MODEL / MULTIPLE MANUFACTURERS
“The UK Government has allocated £18.5 million to Imperial College London for its vaccine project. Having completed clinical trials, Imperial announced on 17 July 2020 that it was proceeding to the next trial phase, involving 105 participants aged 18-75.
“Imperial has formed a new social enterprise, VacEquity Global Health, to rapidly develop this vaccine and distribute it as widely as possible in the UK and overseas, including to low- and middle-income countries. This is in partnership with Morningside Ventures, a fund based in Hong Kong that invests in companies for the public good.
“Rather than partnering with one company, the Imperial model envisages links with multiple manufacturers and waiving royalties and charging a modest amount for its vaccine. Agreements to purchase, manufacture and distribute the vaccine are still being negotiated.”
ANOTHER DOSE OF VACCINES
RUSSIA SETS MASS VACCINATION FOR OCTOBER AFTER SHORTENED TRIAL
Russia plans to launch a nationwide vaccination campaign in October with a coronavirus vaccine that has yet to complete Phase 3 clinical trials.
Comment from Professor Oxford, The Gamaleya is a famous immunology Institute full of expertise; it is not a little USA biotech. So, I am taking them seriously. I like their target groups viz armed forces and teachers. Both the Oxford group and the Gamaleya Institute are using well established adenovirus vectors. The Gamaleya has experience in both vaccine design and manufacture and works well with the government control institute.
OXFORD VACCINE TRIAL REPORT
Reported in The Lancet No serious adverse effects. Acetaminophen (aka paracetamol) reduced any mild effects. Neutralising antibodies induced in all participants after second dose. After two doses, potent cellular and humoral immunogenicity was present in all participants studied.
“These results, together with the induction of both humoral and cellular immune responses, support large-scale evaluation of this candidate vaccine in an ongoing Phase 3 programme.”
WUHAN CANSINO TRIAL REPORT
Reported in The Lancet This was the first double-blind, placebo controlled, Phase 2 trial of the CanSino vaccine had 508 randomised participants of a single dose, half dose, or placebo. Seroconversion (antibody) development was similar with full or half dose (96% (95% CI 93-98) and 97% (92-99), respectively, at day 28). No serious adverse reactions were documented.
DOES NORTH KOREA HAVE A VACCINE?
The socially-isolated nation claims to have zero coronavirus cases, but this week, its State Commission of Science and Technology announced clinical trials for its domestic vaccine candidate were underway. There are many who find these claims dubious. As one of the world’s poorest nations, North Korea has relied for decades upon the UN for immunisations.
MRNA VACCINE WITH ROBUST IMMUNE RESPONSE, INCLUDING CD4, CD8, IN MICE
“Here, we provide a detailed evaluation of the immunogenicity of lipid nanoparticle-encapsulated, nucleoside-modified mRNA (mRNA-LNP) vaccines encoding the full-length SARSCoV-2 spike protein or the spike receptor binding domain in mice.
“We demonstrate that a single dose of these vaccines induces strong type 1 CD4+ and CD8+ T cell responses, as well as long-lived plasma and memory B cell responses.
“Additionally, we detect robust and sustained neutralising antibody responses and the antibodies elicited by nucleoside-modified mRNA vaccines do not show antibody-dependent enhancement of infection in vitro.
“Our findings suggest that the nucleoside-modified mRNA-LNP vaccine platform can induce robust immune responses and is a promising candidate to combat COVID-19.”
“TWEETORIAL” ON PRE-EXISTING IMMUNITY BY @ADAMKUCHARSKI
Mathematician/Epidemiologist at London School of Hygiene & Tropical Medicine
Welcome Trust Fellow, TED Fellow (“A global network of trailblazers, changing the world”)
Author of “The Rules of Contagion”
How much could pre-existing immunity affect the dynamics of COVID-19?
To answer this question, it is useful to look at two similar but subtly different concepts – the “reproduction number, R” and the “basic reproduction number, R0”…
R is the average number of secondary infections generated by a typical infectious person, so reflects both social behaviour and susceptibility within a population. In contrast, R0 is expected number of secondary infections if everyone in population were fully susceptible.
There’s more on the relationship between the two in my talk here (from 27:00): newton.ac.uk/seminar/202007…. But why is this distinction important?
If we are re-calculating the impact of immunity, R0 is the crucial value. Suppose, hypothetically, that 50% of a population is not susceptible to an infection. If observed R is 3, it would mean the R0 is much higher (because R is 3 despite only half population being susceptible).
So, if we are calculating how much effect pre-existing or acquired immunity might have on an epidemic, we have to first estimate what R0 would be (i.e. in the absence of any immunity). If we use the observed value of R instead, we risk double counting the effects of immunity.
Punchline: if you think some groups are less susceptible to SARS-CoV-2, then it is important to adjust for this and use the larger R0 value when discussing hypothetical dynamics of immunity.
International SOS Comment: Pre-existing immunity must be controlled for in Phase 3 vaccine trials.
PRE-EXISTING IMMUNITY
LET’S REMEMBER THE CAUSES OF THE COMMON COLD
The common cold is a viral infection of the upper respiratory tract. The most commonly implicated viruses are:
- Rhinovirus (30–80%) with 99 known serotypes
- Human coronaviruses (≈ 15%)
- Influenza viruses (10–15%)
- Adenoviruses (5%)
The four human coronaviruses that generally produce mild symptoms are:
- Human coronavirus OC43 (HCoV-OC43), β-CoV
- Human coronavirus HKU1 (HCoV-HKU1), β-CoV
- Human coronavirus 229E (HCoV-229E), α-CoV
- Human coronavirus NL63 (HCoV-NL63), α-CoV
THE CORONAVIRUS IS NEW, BUT YOUR IMMUNE SYSTEM MIGHT STILL RECOGNISE IT
Forty percent of people with coronavirus infections have no symptoms. Might they be the key to ending the pandemic?
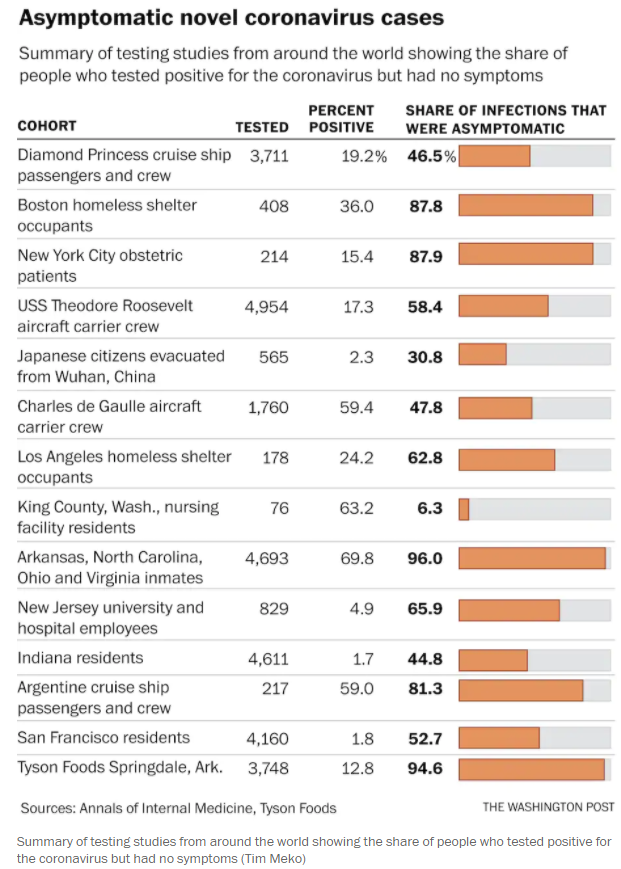
Recent studies have revealed that 20-50% of people in some places may have T cells that recognise SARS-CoV-2 despite having never encountered it before.
Study 1; Study 2; Study 3; Study 4.
These T cells were most likely produced from past infections with the four coronaviruses that frequently cause common colds. The significance of these T cells is not yet clear (helpful, harmful, or negligible) in a person’s and the role in the world’s fight against the current coronavirus. But should these so-called cross-reactive T cells exert even a modest influence on the body’s immune response to the new coronavirus, they might make the disease milder and perhaps partly explain why some infected people become very sick, while others have few or no symptoms. They would also indicate that immunity to coronaviruses can be long-lasting.
Source: Washington Post
MIS / DISINFORMATION / FAKE NEWS
A CENTURY OF NO CHANGE: THE MASK SLACKERS OF THE 1918 PANDEMIC
An excellent article in the New Daily:
“The masks were called muzzles, germ shields and dirt traps. They gave people a “piglike snout”. Some people snipped holes in their masks to smoke cigars. Others fastened them to dogs in mockery. Bandits used them to rob banks.
“More than a century ago, during the 1918 influenza pandemic, masks of gauze and cheesecloth became the facial front lines in the battle against the virus. But as they have now, the masks also stoked political division.

“Then, as now, medical authorities urged the wearing of masks to help slow the spread of the disease. And then, as now, some people resisted.
“In 1918 and 1919, as bars, saloons, restaurants, theatres and schools were closed, masks became a scapegoat, a symbol of government overreach, inspiring protests, petitions and defiant bare-face gatherings.
“By the fall of 1918, seven cities – San Francisco, Seattle, Oakland, Sacramento, Denver, Indianapolis and Pasadena, California – had put in effect mandatory face mask laws, said Dr Howard Markel, a historian of epidemics and the author of Quarantine! Organised resistance to mask wearing was not common, Dr Markel said, but it was present. “There were flare-ups, there were scuffles and there were occasional groups, like the Anti-Mask League,’”he said, “but that is the exception rather than the rule.”
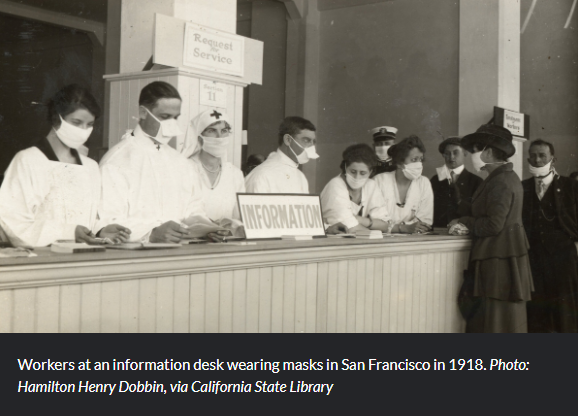
“At the forefront of the safety measures was San Francisco, where a man returning from a trip to Chicago apparently carried the virus home, research archives show.”
“By the end of October, there were more than 60,000 cases statewide, with 7,000 in San Francisco. It soon became known as the ‘masked city”.
“Alma Whitaker, writing in The Los Angeles Times on 22 October 1918, reviewed masks’ impact on society and celebrity, saying famous people shunned them because it was ‘so horrid’ to go unrecognised. ‘The big restaurants are the funniest sights, with all the waiters and diners masked, the latter just raising their screen to pop in a mouthful of food,’ she wrote. When Whitaker declined to wear one, she was ‘forcibly taken’ to the Red Cross as a “slacker” and ordered to make one and put it on.”
DARK MONEY AND PACs **
Two weeks ago, in this Executive Summary, I included links to Dr. Stella Emmanuel and a group of doctors standing in front of the US Capitol claiming, without evidence, that the coronavirus could be cured and that widely accepted efforts to slow its spread were unnecessary and dangerous.

Several readers asked why I had included these links and I realised that I had not explained their relevance sufficiently.
NBC News reports “that the so-called ‘news conference’ had more speakers than attendees was of little matter. Livestreamed by the far-right website Breitbart News, the video spread quickly, initially through conservative, anti-vaccination and government conspiracy groups. Within hours, it had reached over 20 million Facebook users.
It was re-tweeted by Donald Trump Jnr (who had his twitter account suspended for 12 hours) and by President Trump. LINK

“The event was hosted and funded by the ‘Tea Party Patriots’, a right-wing political non-profit group led by Jenny Beth Martin, the group’s co-founder, who spoke at the news conference. The group, which collects funds through two nonprofit groups and a political action committee, has raised over $24 million since 2014 to support Republican causes and candidates.
“The virality of the video underscores the difficulty in moderating coronavirus misinformation as treatments and public health responses have become more political.”
** A “PAC” is a Political Action Committee that pools campaign contributions from members and donates those funds to campaigns for or against candidates, ballot initiatives, or legislation.
COVID-19: ONLY HALF OF BRITONS WOULD DEFINITELY HAVE VACCINATION
A group of scientists and pollsters have found that only 53% said they would be “certain” or “very likely” to allow themselves to be given a vaccine against the disease if one becomes available.
By contrast, one in six (16%) said they would definitely not or would be unlikely to accept a vaccine, according to research by King’s College London and Ipsos MORI.
In addition, it was found that one in five (20%) said they would only be “fairly likely” to go ahead with vaccination.
The study found vaccine rejection was strongest among those whose beliefs reflect greater scepticism about science and who are less concerned about the impact of the C pandemic. Likely refusal was also linked to those who tended to be less willing to wear face masks and who said they got most of their information about the disease from WhatsApp and other social media outlets.
There was also a significant age divide in responses with 22% of those in the 16-24 and 25-34 age groups saying they would be unlikely or definitely would not accept a vaccine compared with only 11% among 55-75 year-olds.
STUDY: 13% OF BRITONS BELIEVE THAT “THE GOVERNMENT ONLY WANTS US TO WEAR FACE MASKS AS A WAY OF CONTROLLING US”
A new study by King’s College London and Ipsos MORI, a pollster, found that 13% of Britons believe that “the government only wants us to wear face masks as a way of controlling us”, and that 18% are “more focused on protecting civil liberties” than controlling the coronavirus.
.
The Daily Telegraph, a conservative broadsheet, has run several pieces decrying their use, arguing that masks destroy public confidence, make their wearers feel “less human” and prove that Britain is “the scaredy-cat of Europe”. A letter-writer to the paper called mandatory mask-use “a massive infringement of my personal liberty”. Toby Young, founder of the Free Speech Union, calls the decision to require people to wear masks “very disappointing”.
Source: Economist
DELTA BANS ANTI-MASKERS
Delta has banned 100 anti-maskers from taking their flights and added them to a “no fly” list. Despite outrage from some consumers, legal experts say it’s within the airline’s scope of rights.
AIR IN THE HOSPITAL ROOM OF COVID-19 PATIENTS IS INFECTIOUS
Researchers in Florida, USA, have taken air samples from the room of two patients with COVID-19. The hospital room had SIX air changes per hour. Air was filtered and irradiated, with 90% being recirculated into the room.
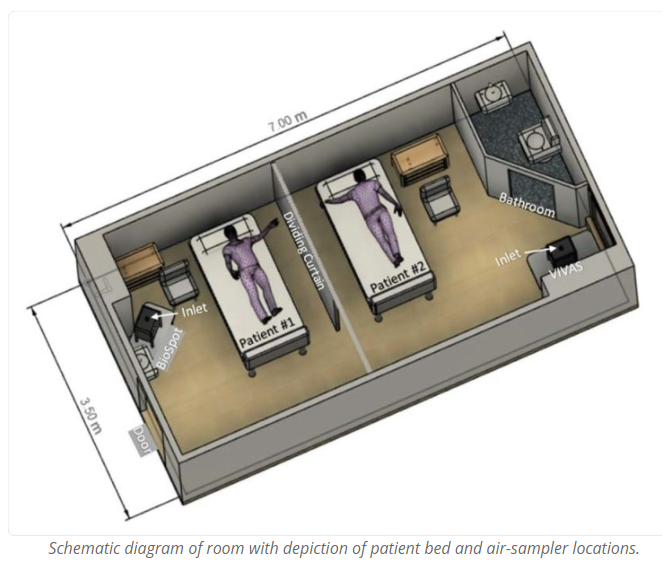
SARS-CoV-2 was found in samples collected 2 to 4.8 metres away from the patients. The virus they collected could experimentally infect cells.
“These findings strengthen the notion that airborne transmission of viable SARS-CoV-2 is likely and plays a critical role in the spread of COVID-19.”
The study is not yet peer-reviewed.
JOURNAL / ARTICLE / TWITTER ROUNDUP
Florida hospitals stretched to capacity by acute coronavirus outbreak
Is the Subway Risky? It May Be Safer Than You Think
More today on lung fibrosis after severe #COVID19
South Korean Shincheonji sect leader arrested
Your facemask should not have a valve Consider taping it up
Sweden urges employees to keep working from home throughout autumn
A VIEW FROM THE LABORATORY: PROFESSOR JOHN OXFORD
HAVE VIRUS EXPERTS IN THE UK BEEN PUSHED ASIDE?
Seventy clinical virologists have written to the Chief Medical and Chief Scientist to say that COVID testing contracts are being awarded to private sector companies who have little expertise or experience. Clinical virologists often work in diagnostic laboratories across the UK and they say that they are not being engaged to apply this experience to questions of utility of new diagnostics. This is a pity and shows lack of knowledge at the centre of COVID planning. Recently two companies have been awarded contracts for a “90-minute test”. But have kits been properly investigated or is it yet another “UK world beating discovery”, which could turn out considerably less effective than expected? Professor Deenan Pillay at UCL has been quoted as saying “it’s almost as if new tests are pushed as a magic bullet, to reassure the public rather than doing contact tracing.” Contact tracing particularly is at the centre of controversy. The new scheme is not working as expected and everyone agrees that such data is needed to inform quickly of new outbreaks, particularly as we approach the time of school re-openings (see below). I suspect myself that “privatization” is a keen word for some politicians.
Sir Jeremy Farrer, Director of the Wellcome Trust in the UK discussed these and other issues in the Sunday Observer; “One thing is clear, reopening schools must be our priority.” He notes that as we head towards autumn, we will be forced to make hard choices to keep transmissions down whilst restarting the economy and protecting public health. He notes that there is no such thing as zero risk. He feels that “testing” is at the centre of improving contact tracing. Whilst cases are identified, they also need to be precisely located in the community. Whether people who are identified have symptoms or not, they need to be tested for virus RNA quickly. “The test, trace and isolate system has to work and deserves all our support.” A simple trade off might be to close our restaurants/pubs where we know many infections are centred.
COVID-19 IN CHILDREN AND THE PRACTICAL QUESTION OF SCHOOL RE-OPENINGS
An important conundrum has always been the role of children spreading respiratory viruses. Influenza evidence points towards children as spreaders of infection in the family. Indeed, we all accepted that children (with poor hygiene and little social distancing) initiated infection in a family group.
From this emerged a preventative vaccine scheme to vaccinate children to help them avoid influenza and at the same time protect the grandparents. This logic came from early studies in Japan which showed protective effects of flu vaccine in a family group where the children had been vaccinated.
The same data came from Michigan in the USA. And so, for the last 4-5 years in the UK we have given children live attenuated influenza vaccine. Indeed, the initial data, and the current data, support the hypothesis.
But what about COVID?
Would it have the same characteristics?
Some data with antibody testing with COVID-19 suggests a more complicated spread. Antibody testing by A. Fontanet and colleagues (at the Institute Pasteur) at an outbreak near Paris noted a difference in incidence between secondary and primary schools. Around 40% of students and staff in secondary schools had antibody where only 8% or so of teachers and children in primary schools had been infected. Certainly, virological data from Berlin had shown that the quantity of virus present in these different groups is not so different. Of course, the younger children are often asymptomatic, and this may explain the reduced infection.
For many countries which find themselves planning to re-open schools, the strategy may now be not as clear as we would have liked. Also, the new virus may be more prone to spread in virus clusters.
The UK government has introduced guidelines. An idea is to break down classes into subgroups or “bubbles”. In Denmark the pupils in a bubble would wash their hands every two hours and sit 1½ metres apart. Scottish schools open on this Monday and soon we will have their personal experience at hand.
VIEWS FROM AFRICA AND AUSTRALIA
When I worked in Canberra as a virologist, my family and I would often drive for 80 miles to “the bush”. There we stayed at a large sheep farm. The owner rented out horses and they were our objective.
But sheep came into the equation when one year a group of itinerant Australian sheep shearers arrived. They stayed on the farm for a week and we ate lamb for every meal, even breakfast. I noted today that Australia still has 60 million sheep but this year COVID has intervened.
Hundreds of New Zealand shearers usually arrive in August to help alongside 3,000 or so Australian experts. Two animal welfare issues are for the sheep to be sheared BEFORE lambing and secondary “fly strike”, where blow flies lay eggs and then affected sheep may have to be killed. But who will pay for quarantine of the shearer? Similarly, New Zealand may face a shortage of shearers in November.
In Africa, a five-week lockdown has been working but has been ruinous for three million Africans who have lost their jobs. Salim Karim was interviewed for Nature (30 July 2020). He is Chair of the Health Ministry’s Advisors Committee. He describes the tradition of communities looking after each other and could be key to the country’s response. Many informal settlements are poorly supplied with water. He is seeing 6,000 new cases each day near Johannesburg. But he is surprised that there are not more cases. He mentions the word “ubuntu” – “I am because you are”. In other words, safety is interdependent and can push a change in people’s behaviour. We as a country are built on the principle of “I am because you are” and we have to rediscover that, as we wait to defeat this virus!
THE RISKY THREAT FROM ANIMAL VIRUSES
A research project has assessed 7,000 animal communities on six continents. Significantly, from the point of view of infection, conversion of wild areas into farmland destroyed large sized animal species but small animals, many of which can carry pathogens, benefitted. The report notes that disease surveillance needs to be increased in the areas where nature is being destroyed. Dr Redding a co-author and worker at the ZSL Institute of Zoology in London noted that small perching birds do well under these conditions. An emerging disease has been West Nile virus. Fast living species such as brown rats carry a range of diseases. They are small, mobile, adaptable and produce lots of offspring rapidly.
THE GOLDEN HAMSTER AS A MODEL INFECTION FOR COVID-19
Even in these days of molecular biology, gene sequencing and natural construction of viruses, a good animal model can throw light on pathogenesis as well as virus transmission. A group from Hong Kong including Malik Peiris describe a good model in Nature (Sin Fun Sia et al. Nature, 585, 836, 2020).
It is not a perfect model because the curious immunopathology seen in patients is not reproduced. Rather the animals develop upper and lower respiratory tract infection. There is lung consolidation after 2-5 days followed by clearance of virus. Virus RNA was detected from 14 days in the respiratory tract but virus itself was short lived and correlated with infectibility for other animals. Animals lost weight but did not die and recovered and produced antibody. So, the model is one of mild coronavirus. This can be very useful to study vaccine efficacy. After all, most infections in humans are mild.
Mice can be infected if a gene from the ACE receptor is cloned into them. The golden hamster has been used for SARS virus. In these experiments the animals are infected intranasally with around 100,000 infective doses of a virus isolated Vero EG cells. Histopathology showed inflammatory cells and consolidation in 5-10% of lungs at two days post infection. There was moderate inflammatory cell infiltration in nasal turbinate’s and olfactory sensory neurones. Given the loss of taste and smell in many patients, this will need more extensive study.
No histological changes were seen in the brain, heart, liver and kidney. Importantly, the virus could be transmitted by aerosol. I feel that the model will be useful for screening new vaccines for safety and effectiveness and I have a soft spot for Mesocricetus auratus (the golden hamster) from my student days!
There are not so many diagnostic reagents available for hamsters as for mice but the next months could still be very fruitful for new data.
AUTHORS
Dr Quarry MBBS, MSc (Community Health), Group Medical Director, Health Intelligence, International SOS
Professor John Oxford PhD, DSc, FRCPE, International Virologist & Author, Blizzard Institute, Queen Mary College, London., Scientific Director, Oxford Media Medicine

Think Different. Think DouglasNews.Network.
Your support matters. Support from our readers helps protect our editorial independence. Help us to report fearlessly on issues that affect our region, and to challenge those in power. Help us continue to deliver quality, trustworthy, fact-checked journalism that is free to access.



